5.3.2. Cups BICON Plus POROSE
5.3.2.1. The reasons for creating Bicon Porose cups
In the case of a patient whose bone is porotic, an operator currently using cementless cup may doubt the reliability of cementless fixation and consider implantation of a cemented cup.
This attitude was perfectly justified in the case of certain cementless cups for which he knew in advance that primary stability was not guaranteed in poor quality bone. This was also the case for cementless cups which did not have sufficient grip in the cancellous bone and which required additional screws, or the case for screwed cups whose thread was thick, or tight or too shallow. Likewise, most of the impacted spherical cups left the same uncertainty in a bone whose ability to secondary regrowth was improbable.
One of the risks of failure of acetabular cups without cement screwed into porotic bone was the destruction, by excessive screwing force, of the thread which had just been cut into the porotic bone bed, therefore not very resistant due to lack of end of screwing mark.
Another risk of failure was the excessive rigidity of the shells in an environment that was also more flexible than in a normal bone, with the already rarefied bony trabeculae collapsing when a slightly strong load occurs.
It was the knowledge of these widely published problems that led me to think about solutions to reliably implant a screwed metal shell in a porotic acetabulum.
In 1973, I participated in a study on osteoporosis in Doctor Duriez's Bone Disease Research Center at the Calot Institute in Berck-Plage, in which I had installed a Zeiss Micro VideoMat system connected to a computer that I had specially programmed.
Reflections and intraoperative observations allowed me to make modifications to a screwed shell without cement, already reliable in hard bone, to obtain a result of equivalent reliability in porotic bone.
5.3.2.2. Increase in tooth surface area
In order for the osteoporosis implant to support a greater number of bony sections of the already rarefied structure, I significantly enlarged the osseointegrable surface of each wing and, consequently, of the entire implant.

5.3.2.3. Importance of the Operator's tactile sensations during screwdriving
I made several modifications to the structure of the wings of the hard bone Bicon shell, to prevent excessive screwing into porotic bone and increase screwing resistance so that the operator has an almost unchanged screwing sensation compared to the hard bone shell and easily detects the resistance at the end of screwing.
5.3.2.4. Decreased tooth attack angle
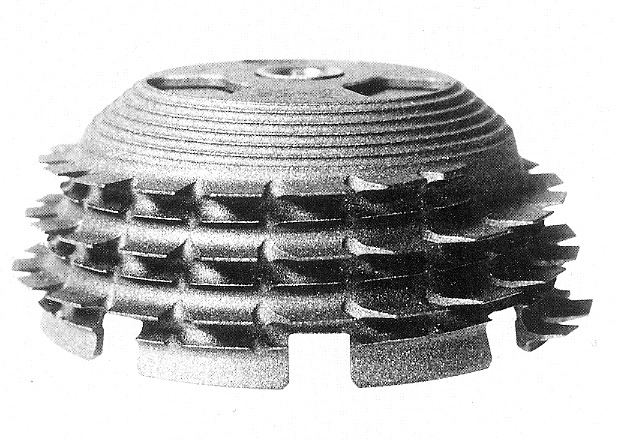
This angle of attack, quite aggressive for the hard bone shell, made it look like a circular saw. For porotic bone, this cutting ability would have been excessive. The angle of attack has therefore been greatly reduced.
5.3.2.5. Increase in radial tooth length
The length of the Porotic Bone Shell teeth has been increased by approximately 30%.
5.3.2.6. Increased tooth length
5.3.2.7. Reduction in tooth misalignment
The notion of "decalibration", well known to mechanics, consists of reducing the length of a tooth of the cup on the side opposite the cutting tip to eliminate the braking effect in the furrow that this tip has just dug.
The "decalibration" applied to the teeth of the shell for hard bone has been almost eliminated on the teeth of the shell for porotic bone precisely in order to increase friction during screwing.
5.3.2.8. Decrease in thickness at the tips of the teeth
The thickness of the tip of the teeth of the Porose shell has been reduced with the aim of increasing their flexibility in a rarefied structure of spongy bone, to yield elastically in the event of micro-movements of the spongy environment, instead of break the trabecular structure.
5.3.2.9. The function of secondary teeth
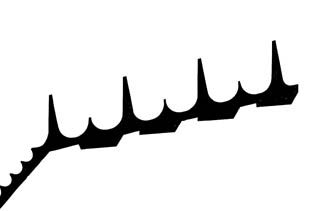
In order to further increase the macrostructure facing a weakened cancellous bone, I found it necessary to create an additional family of teeth whose height reaches 1/3 that of the main teeth. These teeth also have a role in compressing the spongy bone at the end of implantation and constitute an additional primer for regenerating a new trabecular structure. These secondary teeth also contribute to the overall increase in surface area of the acetabulum for porotic bone.
5.3.2.10. The macrostructure of the frontal region
I did not retain the fine macrostructure of the frontal bicone of the hard bone shell because a macrostructure less than a millimeter has practically no effect of increasing surface area and does not contribute to primary stability. Rather, it has a microstructural role during osseointegration. For the shell for porotic bone, the circular grooves of the small biconical surface have been widened to obtain a real compression and indentation effect already useful for primary fixation.
5.3.2.11. Increase in axial pitch of main teeth
The axial screw pitch of the Porose shell has been increased to allow the main teeth to move away from the lower secondary teeth. This prevents the tooth system from only behaving as a macrostructure and risking crushing the spongy bone encountered, the role of the main teeth being more to embed themselves in the rarefied bone without breaking all the bony trabeculae.
A favorable consequence of the modification of the axial pitch is to further increase the resistance to screwing compared to the hard bone shell.
The screwing force is increased by 15%, as analyzed in the discussion in paragraph 5.3.1.7.
All the modifications described previously (angle of attack, offset, length of teeth) were decided to obtain an increase in the surface area of the fins.
5.3.2.12. Calculation of tooth surface variation
For a presentation, to demonstrate the advantage of the Porose shell in a porotic acetabulum, and to compare it to the shell for hard bone, I programmed the calculation with good precision of the total surface of the teeth, to all sizes.
These calculations gave the following surfaces for the teeth of the two types of shells:
5.3.2.13. The Porose shell in reoperations
It quickly became apparent that the Porose shell could often be very advantageous for acetabulum reoperations. After extraction of a cemented acetabulum and removal of cement from the surface of the acetabulum, the overall shape of the cavity is often far from a perfect half-sphere and the thin layer of cortical bone has been partially penetrated. The ability for bone regrowth was weakened by the residual toxic effects of cementing.
For reoperations, the Porose shell provides an excellent solution. Its elongated fins allow, with a single economical milling preparation, to remove only the parts which could come into conflict with the main body of the cup.
I find that it would be wrong, in order to have perfect contact at all points of the shell, to resize the bone by sacrificing what still remains of resistant bone, and to implant a very large size.
The elongated wings make it possible to establish a bridge where bone is missing and to reach all points of the bone structure whatever its condition. The large number of support points allows the Porose shell to be sufficiently immobilized so that no screws or additional stabilization systems are necessary.
The teeth of the Porose shell present an intimately encrusted surface facing the bone which is ten to twenty times greater than that offered by several cancellous bone screws whose thread surface only reaches around a hundred square millimeters per screw.
The remarkable properties of overall flexibility of the shell, and local flexibility of the teeth, always promote medium-term regrowth of the bone structure, and avoid breaking bone structures still intact after reoperation.
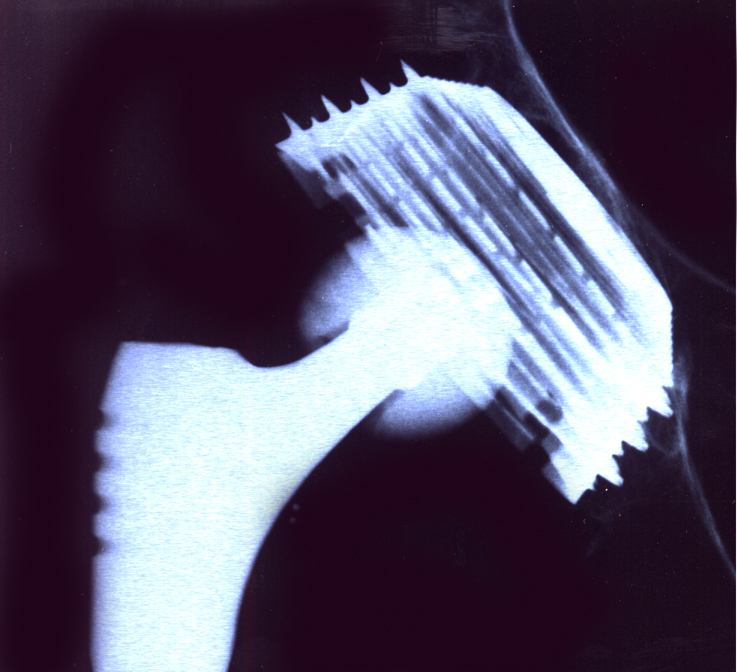
In cases of reoperations, the thin Titanium shell plays the role of a “cortical prosthesis” in the architecture of the acetabulum. In the medium term, the trabecular structure is reconstituted around the titanium shell and all of the fins without a new millimetric layer of compact bone forming. I would be grateful to receive from readers radiographs which confirm this "cortical prosthesis" effect of the thin shell.

Only a screwed acetabulum with wings could be adapted to the porotic bone. I cannot imagine how impacted and press-fit shells could have received modifications making them suitable for unchanged stability in porotic bone.
----
Next implant: